The UCSF-John Muir Health Jean and Ken Hofmann Cancer Center at the Behring Pavilion is now open. LEARN MORE >
What is the thyroid?
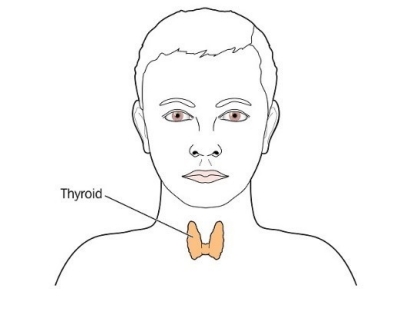
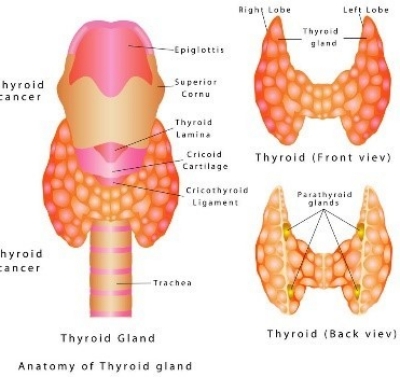
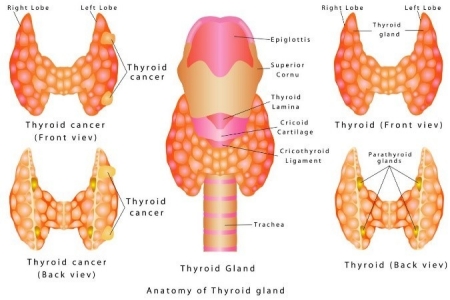
The thyroid gland is one of the body's most important endocrine organs located at the lower part of your neck, just below your Adam’s apple. It is shaped like a butterfly – each wing, or lobe of your thyroid lies on either side of your windpipe.
What is the function of thyroid?
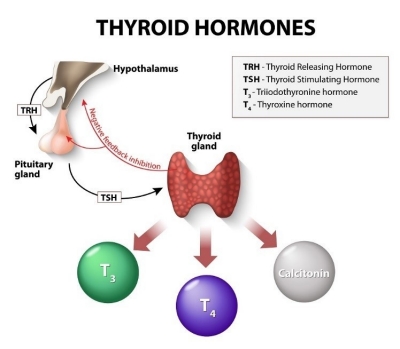
The purpose of your thyroid gland is to make, store, and release thyroid hormones into your blood. These hormones affect almost every cell in your body, and help control your body’s functions. If you have too little thyroid hormone in your blood, your body slows down. This condition is called hypothyroidism. If you have too much thyroid hormone in your blood, your body speeds up. This condition is called hyperthyroidism.
Thyroid Diseases
Hypothyroidism
Hypothyroidism is usually associated with decreased production of hormone in the thyroid gland. Lack of iodine intake can also result in hypothyroidism in certain countries. Other causes of hypothyroidism include Hashimoto’s thyroiditis, radioactive iodine therapy, and medication induced and surgery.
Goiter (endemic, multinodular)
Mild to moderate iron deficiency still exists in many parts of the world. Iron deficiency can result in a preventable endemic goiter. Multinodular goiter is described as diffusely enlarged thyroid gland that is often associated with nodularity that can be asymmetrical. With goiter a person can have normal thyroid levels or become hyperthyroid. Incidence of thyroid cancer in nodular goiter is reported between 5-9% and biopsy of suspicious nodules should be considered.
Thyroiditis
Thyroiditis is associated with inflammation or infection of the thyroid gland. Hashimoto’s thyroiditis is a major cause of hypothyroidism in the United States which results in altered thyroid hormone production and hypothyroidism. Acute thyroiditis is very rate and is the result of infection of upper airway and thyroid gland causing severe localized pain. The exact cause of subacute thyroiditis is not known but is associated with viral disease. It can also present as swelling of thyroid gland, pain, fever and fatigue. Treatment of thyroiditis is variable depending on the etiology of the disease.
Hyperthyroidism/Graves'
Graves’ disease is one of the most common causes of hyperthyroidism. Other causes of hyperthyroidism include nodular goiter, thyroid adenomas and central nervous system disease. Increased heart rate, abnormal heart rate, sweating, weight loss, heat intolerance, hair loss and menstrual changes are some of the manifestations of hyperthyroid state. The main treatment options for hyperthyroidism include anti-thyroid medications, radioactive iodine therapy and surgery.
Thyroid cancer
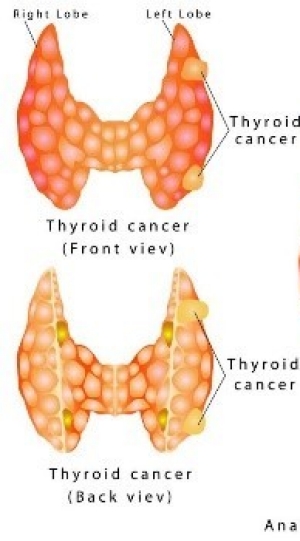
The incidence of thyroid cancer in the United States is increasing. In United states more than 60,000 new cases of thyroid cancer were predicted for 2014 compared to less than 40,000 in 2009.
Papillary
Papillary thyroid cancer is the most common type of thyroid cancer making more than 90% of all thyroid cancers. It is more common in in women, and usually presents as a thyroid nodule or a slow growing neck mass with normal hormone levels. Lymph node metastasis is common in papillary thyroid cancer especially in younger patients and could be a presenting symptom. Overall survival in papillary thyroid cancer is excellent with >95% ten year survival rate.
Follicular thyroid cancer (FTC)
Incidence of follicular carcinoma in the United States is decreasing and it accounts for less than 10% of thyroid cancers. It is a disease presenting in persons over the age of 50, and is more common in women. Follicular carcinoma usually presents as a solitary nodule and can spread through the circulatory system to distant sites.
Hurthle cell thyroid cancer
It is considered to be a subtype of follicular cancer and some studies suggest higher rate of recurrence.
Medullary thyroid cancer
Medullary thyroid cancer (MTC) accounts for a small portion of thyroid cancers. It arises from the parafollicular or C-cells in the thyroid which produce the hormone calcitonin. This hormone functions to lower the blood levels of calcium. Patients with MTC usually have elevated levels of calcitonin and/or carcinoembryonic antigen (CEA). High level of these hormones is associated with systemic symptoms such as diarrhea.
Anaplastic /Poorly differentiated
Anaplastic thyroid cancer accounts for less than 1% of all thyroid cancer in the United States. As with other types of thyroid cancer, it is more common in women and presents at older age as a rapidly growing neck mass in the setting of goiter. Difficulty breathing or swallowing, and voice changes may also be present. Multimodal therapy including surgery should be considered when possible.
Other
Metastatic disease to the thyroid from other cancers such as kidneys, breast, lung and melanoma has been reported. Lymphoma can also occur in the thyroid on rare cases. It accounts for about 1-5% of thyroid malignancies and is known to grow rapidly.
Thyroid Surgery
Surgery for thyroid cancer
Surgery is the main treatment for thyroid cancer, except for some anaplastic thyroid cancers. If thyroid cancer is diagnosed, surgery to remove part or all of the thyroid gland is usually recommended.
Thyroid lobectomy
This operation may be used to treat different thyroid cancers (papillary or follicular) where the tumor is confined to the thyroid gland and there is no sign of spread beyond the gland. It may also be used as a diagnostic measure in place of a biopsy.
Some patients benefit from not needing to take thyroid hormone pills after surgery since part of the gland is left untouched. Additionally, there is no concern for hypoparathyroidism or low calcium levels since half the gland remains. It may limit interpretation of blood tests (thyroglobulin) used to monitor patients with thyroid cancer after surgery.
Total or near total thyroidectomy
Thyroidectomy is surgery to remove the thyroid gland. As with lobectomy, this is typically done through an incision across the front of the neck. This is the most common surgery for thyroid cancer. If the entire thyroid gland is removed, it is called a total thyroidectomy or near-total thyroidectomy.
After a thyroidectomy you may need additional treatment such as radioactive iodine. You will need to take daily thyroid hormone (levothyroxine) pills.
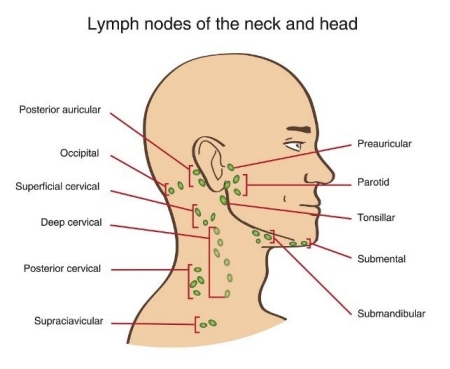
Lymph node removal
If cancer has spread to nearby lymph nodes in the neck, these will be removed at the same time surgery is done on the thyroid. Compartmental removal of the nodes in the central neck (near the thyroid) with or without lateral neck (side of the neck) is the treatment of choice.
Risks and side effects of surgery
Complications are less likely to happen when the operation is done by an experienced thyroid surgeon. Patients who have thyroid surgery often leave the hospital within a day following the operation. Patients with more extensive surgery such as neck dissection may stay longer at hospital. Potential complications of thyroid surgery include:
- Temporary or permanent hoarseness or loss of voice. This may also occur if the nerves to the vocal cord (recurrent laryngeal nerve) are damaged during surgery. Examination of vocal cords before or after surgery may be performed. Irritation to the trachea and larynx and irritation of the nerves may result in temporary hoarseness of voice.
- Damage to the parathyroid glands (small glands near the thyroid that regulate blood calcium levels). This can lead to low blood calcium levels, causing numbness and tingling sensations around the mouth and fingertips and muscle spasms.
- Bleeding or formation of a large blood clot in the neck (hematoma).
- Wound infection.
The parathyroid glands are four tiny glands, located in the neck behind your thyroid gland, that control the body's calcium levels. Each gland is about the size of a grain of rice (weighing approximately 30 milligrams and is 3-4 millimeters in diameter).
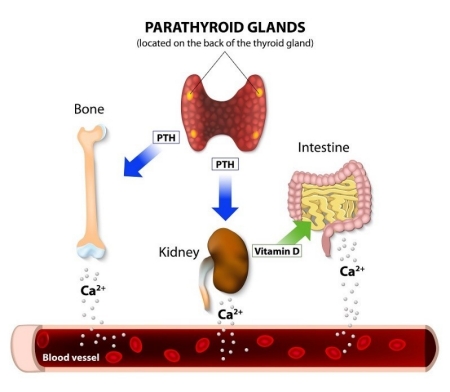
Parathyroid glands control your body calcium level through bone, intestine and kidneys. They are responsible for producing parathyroid hormone (PTH) which regulates the circulating level of calcium. It has direct action on bones and kidneys with indirect effects on intestinal tracts through vitamin D metabolism.
Parathyroid Diseases
Primary Hyperparathyroidism (PHPT):
PHPT is usually diagnosed by a doctor through hypercalcemia found on routine laboratory results with elevated levels of parathyroid hormone (PTH). Patients with PHPT typically have low phosphorus, due to elevated PTH levels which decrease the resorption of phosphorus in the kidneys. Most commonly, these patients are asymptomatic; however, a careful history and physical examination is necessary to rule out other causes of hypercalcemia. Other causes of hypercalcemia include conditions such as metastatic cancer, multiple myeloma, sarcoidosis and other granulomatous diseases, ingestion of calcium or vitamin D, milk-alkali syndrome, and other less common causes.
Secondary Hyperparathyroidism:
Secondary hyperparathyroidism is caused by chronic over stimulation of the normal parathyroid glands usually in the setting of chronic renal failure (kidney disease). This is a result of a complex set of interactions, including a decrease in renal failure conversion of vitamin D to its active form resulting in decreased intestinal absorption of calcium and PTH levels increase, and in mobilization of calcium from bone. Also elevated levels of phosphorus results in further stimulation of the parathyroid glands. Secondary HPTH can also result from malabsorption in the setting of chronic pancreatitis and certain types of bariatric surgery. Treatment of the underlying cause of the disease such as renal transplant is typically performed, and parathyroidectomy may be required in certain cases.
Tertiary Hyperparathyroidism:
Tertiary hyperparathyroidism occurs when the chronically stimulated parathyroid glands function independent of serum calcium levels. Treatment of choice for tertiary hyperparathyroidism is the surgical removal of three and half glands.
Parathyroid Carcinoma:
The overall incidence of parathyroid carcinoma is very low, and it is difficult to diagnose in part because of its rarity. A small percentage of parathyroid carcinomas present with normal hormone levels. Parathyroid carcinoma occurs with equal frequency in men and women.
Identifying Parathyroid Diseases
Ultrasound
Ultrasound is the most frequent imaging modality used in the evaluation of thyroid and parathyroids.
Sestamibi Scan
Sestamibi (Technetium-99m-methoxyisobutyl isonitrile) scan is a nuclear medicine imaging test used in identifying parathyroid adenoma. Frequently, sestamibi scan is used in conjunction with anatomic imaging such as ultrasound, CT or MRI in evaluating abnormal parathyroid glands.
Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
CT scanning can provide valuable information for the identification of abnormal parathyroid glands in atypical locations. MRI is another anatomic imaging modality used for detecting abnormal parathyroid glands.
Helpful Resources
We use cookies to measure website traffic and personalize content for a better browsing experience. By using this website, you consent to our cookies. For more details, see our Website Privacy Policy.